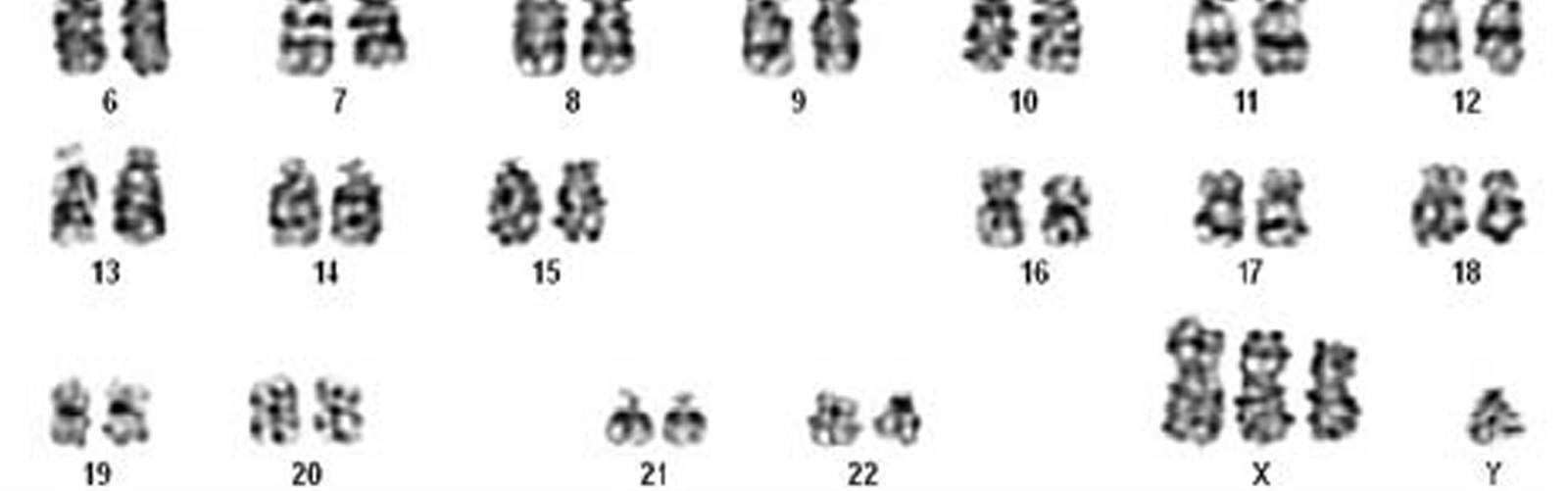
XXXY syndrome is characterised by the presence of three extra X chromosomes in males also known as 48,XXXY.
XXXY syndrome is a genetic disorder characterized by a sex chromosome aneuploidy, where males have two extra X chromosomes. Males typically have only two sex chromosomes, an X and a Y. The presence of one Y chromosome with a functioning SRY gene causes the expression of genes that determine maleness. Because of this, XXXY syndrome only affects males. The additional two X chromosomes in males with XXXY syndrome causes them to have 48 chromosomes, instead of the typical 46. So, XXXY syndrome is often referred to as 48, XXXY.
XXXY syndrome is sometimes referred to as a variant of Klinefelter syndrome/XXY, but differs from Klinefelter syndrome in many ways and is more severe. It is believed by many that individuals with XXXY have their own unique physical and behavioural characteristics and should not be considered a variant of Klinefelter syndrome.
The additional X chromosome in XXXY syndrome has more influence on physical, cognitive and behavioural features than in Klinefelter syndrome/XXY.
Who is affected
An estimated 1 in 17,000 to 50,000 boys are born with XXXY syndrome. XXXY syndrome is a chromosome condition that only affects males. It is rare and there is little specific information available.
Causes
The parents of a son with XXXY syndrome almost always have normal chromosomes in their body’s cells, so they are not routinely tested. Why the two extra X chromosomes were incorporated is not well understood but it is known that they can come from either the mother or the father but not so far as is known from both parents.
A normal female egg contains one X chromosome and normal male sperm contain either one X or one Y chromosome; together they create a fertilised egg with either 46,XY or 46,XX chromosomes. XXXY syndrome usually arises when a Y-bearing sperm fertilises a woman’s egg carrying XXX chromosomes or when sperm with an XXY chromosome make-up fertilise an egg with a single X chromosome.
In the great majority of cases we don’t know why this happens. What is known is that the syndrome arose before conception (when a baby is made) and there is nothing that the parents did before or during pregnancy to make it happen. No environmental, dietary or lifestyle factors are known to cause it. It is no-one’s fault. When boys or men with XXXY syndrome have a mosaic form of the condition, it is likely that a further error occurred in the very earliest days after conception when the embryo is developing.
The likelihood of having two children with XXXY syndrome is extremely rare but It is important to discuss this issue with a genetic counsellor or geneticist because the chance of having another child with a chromosomal condition also depends on several factors such as family history and parental age.
Signs and symptoms
Individuals with XXXY syndrome have a wide spectrum of physical, developmental and behavioural characteristics, ranging from mild to severe. Signs and symptoms of XXXY syndrome can vary but may include learning difficulties; intellectual disability; low muscle tone (hypotonia); hypogonadism; delayed growth and distinctive facial features. Many also have poorly developed social skills and delayed language development.
Boys with XXXY syndrome may have global developmental delay in infancy. If left unaddressed, early speech delays may later manifest in language-based learning disorders, with expressive language slightly more impaired than receptive. Intellectual ability varies, with cognitive abilities falling between mildly bellow normal and within normal limits. XXXY boys’ personalities have been described as shy, sweet, passive, and non-assertive.
Most boys and men with XXXY syndrome their speech and language development are particularly affected. Most affected boys and men can understand what other people say more easily than they themselves can speak. The problems with speech and communication can contribute to behavioural issues, including irritability and outbursts or temper tantrums. Boys and men with XXXY syndrome tend to have anxiety, a short attention span, and impaired social skills.
As a result of early language deficits, they have increased propensity for reading and spelling problems and social difficulties. Their overall IQ may be below their age-matched typical peers, and they are likely to have a lower verbal IQ due to language delay.
XXXY syndrome is also associated with weak muscle tone (hypotonia) and problems with coordination that delay the development of motor skills, such as sitting, standing, and walking. Affected boys and men tend to be taller than their peers, with an average adult height of over 6 feet.
For instance, males with XXXY may have delays in motor skills, language and social development. So early and ongoing intervention and educational planning are critical in ensuring that boys continue to progress in their developmental skills.
Other physical differences associated with XXXY syndrome include abnormal fusion of certain bones in the forearm (radioulnar synostosis), an unusually large range of joint movement (hyperextensibility), elbow abnormalities, curved pinky fingers (fifth finger clinodactyly), and flat feet (pes planus), dental issues (taurodontism). Affected individuals may have distinctive facial features, including widely spaced eyes (ocular hypertelorism), outside corners of the eyes that point upward (up slanting palpebral fissures), and skin folds covering the inner corner of the eyes (epicanthal folds). However, some boys and men with XXXY syndrome do not have these differences in their facial features.
XXXY syndrome disrupts male sexual development. The penis is shorter than usual, and the testes may be undescended, which means they are abnormally located inside the pelvis or abdomen. The testes are small and do not produce enough testosterone, which is the hormone that directs male sexual development. Sexual function is normal, but the shortage of testosterone often leads to incomplete puberty. Starting in adolescence, affected boys and men may have sparse body hair, and some experience breast enlargement (gynecomastia). Their testes typically do not produce sperm, so most men with this condition are infertile.
Diagnosis
Males with XXXY syndrome are diagnosed anywhere from before birth to adulthood as a result of prenatal testing and the range in the severity of symptoms.
Prenatal testing is significantly increasing due to its availability and continued advancements. Many expectant parents are completely unaware that these tests can also identify X & Y sex chromosome variations. These tests can be obtained via analysis of the mother’s blood known as the Harmony test or NIPT. The results can give a percentage of likelihood of an XXXY diagnoses. Diagnoses isn’t confirmed until further testing is obtained. The options available are, the analysis of amniotic fluid via amniocentesis or analysis of tissue samples from a portion of the placenta via chorionic villus sampling (CVS). These tests are invasive and can have a small risk of causing a miscarriage. Expectant parents have the option to wait until the baby is born and confirm a diagnosis through the baby’s blood sample.
A diagnosis of XXXY in children and adults is often made if several of the above signs, symptoms and features are observed. Testing is made based upon a thorough clinical evaluation, a detailed patient history, and specialised blood tests for chromosomal analysis that detect the presence of two extra X chromosome (48,XXXY karyotype). The most common type of testing is a specialised blood test known as karyotyping. Children and adults displaying a combination of speech and language delays, motor delays, difficulty particularly with reading, displaying impulsive and challenging behaviour with attention difficulties and have a tall stature should have a blood karyotyping carried out to confirm or rule out an XXXY diagnoses.
Treatment
There is no cure for XXXY syndrome. Treatment depends on the symptoms present in each individual and is best managed by a team of specialists, including GP, paediatrician, cardiologists, orthopaedists, speech therapists, occupational therapist, physiotherapist, neurologists, and endocrinologists. Life expectancy is generally normal in the absence of major complications. Regular medical visits are often needed, in particular to monitor problems with hormone production, language and developmental delays, and behaviour.
Interventional therapies such as physiotherapy and speech therapy, individual educational plans and ongoing support will maximise the potential of those with XXXY.
Those with XXXY syndrome tend to experience more severe speech delays and should therefore a speech and language assessment, if any deficits are identified they should attend regular speech therapy. This form of therapy helps children/adults to understand and produce more complex language, greatly improving their communication ability and having a positive effect on social interactions.
Since hypotonia is common in those with this syndrome a physical therapy assessment is advised, and if any hypotonia is identified physio therapy should be attended regularly. This form of therapy may help these individuals develop muscle tone and increase balance and coordination.
Treatments exist for the various symptoms associated with XXXY syndrome. Testosterone therapy, which may be given to help individuals through puberty and then for the rest of their lives, has been shown to have positive impacts on health and some individuals show reduced aggressive behaviour. But, this therapy has also been associated with negative side effects: worsening of behaviour, and osteoporosis. Not all individuals are applicable for testosterone therapy, as the best results are often achieved when dosage begins at the initiation of puberty, and these individuals are often diagnosed at a later age, or not at all. It is best to work in collaboration with an Endocrinologist to determine the best testosterone treatment plan.
Dental concerns are very common, when caught early, taurodontism can be treated with a root canal and is often successful. Appropriate planning to avoid taurodontism is possible, but this syndrome must be diagnosed early, which is not common. Taurodontism can often be detected as a symptom of XXXY syndrome before other characteristics develop and can be an early indicator for it. Surgical treatments to correct joint problems, such as hip dysplasia are common, and are often successful alongside physiotherapy.
It is important if any mental health concerns like depression or anxiety are observed these should be followed up quickly with a health professional as they are unlikely to go away without additional support.
A collaborative approach is essential to ensure all health and developmental challenges are addressed early and monitored ongoing.
With proactive management and effective treatment the impacts XXXY has on a child and individuals life can be greatly decreased.
